In previous work, we have shown that outcomes-based reimbursement (OBR), whereby payments to manufacturers are made conditional on achieving and/or sustaining a certain level of patient benefit, can reduce decision uncertainty for Health Technology Assessment (HTA) bodies and accelerate patient access to cell and gene therapies. The administrative burden of such schemes are often cited as a reason why they are rarely applied in practice, and a central component of this administrative burden relates to the collection of outcomes data.
We argue that there are two important factors that need to be in place in order for OBR schemes to be implemented, and both contribute to this administrative burden:
- An appropriate data collection infrastructure (e.g. registry) for collecting outcomes
- A clinical practice that ensures the necessary data is captured and entered into the database or registry
In January 2019, we published a peer-reviewed article detailing a top-level assessment of the existing data collection infrastructure in the therapy areas most likely to see launches of cell or gene therapies over the next five years. We found that oncology is by far the therapy area with the greatest number of cell and gene therapies at the pivotal trial stage, and that the European Society for Blood and Marrow Transplantation (EBMT) registry seems like a potentially promising framework for facilitating OBR in oncology.
The objective
Given the potential benefits of OBR, and the strong pipeline of gene therapies in oncology, we wanted to have a closer look at the EBMT registry. The objective of this exercise is therefore to perform a gap analysis of the EBMT registry to determine its use in practice, and its applicability for facilitating OBR in oncology in the UK.
The deliverable – research methods and findings
Methods
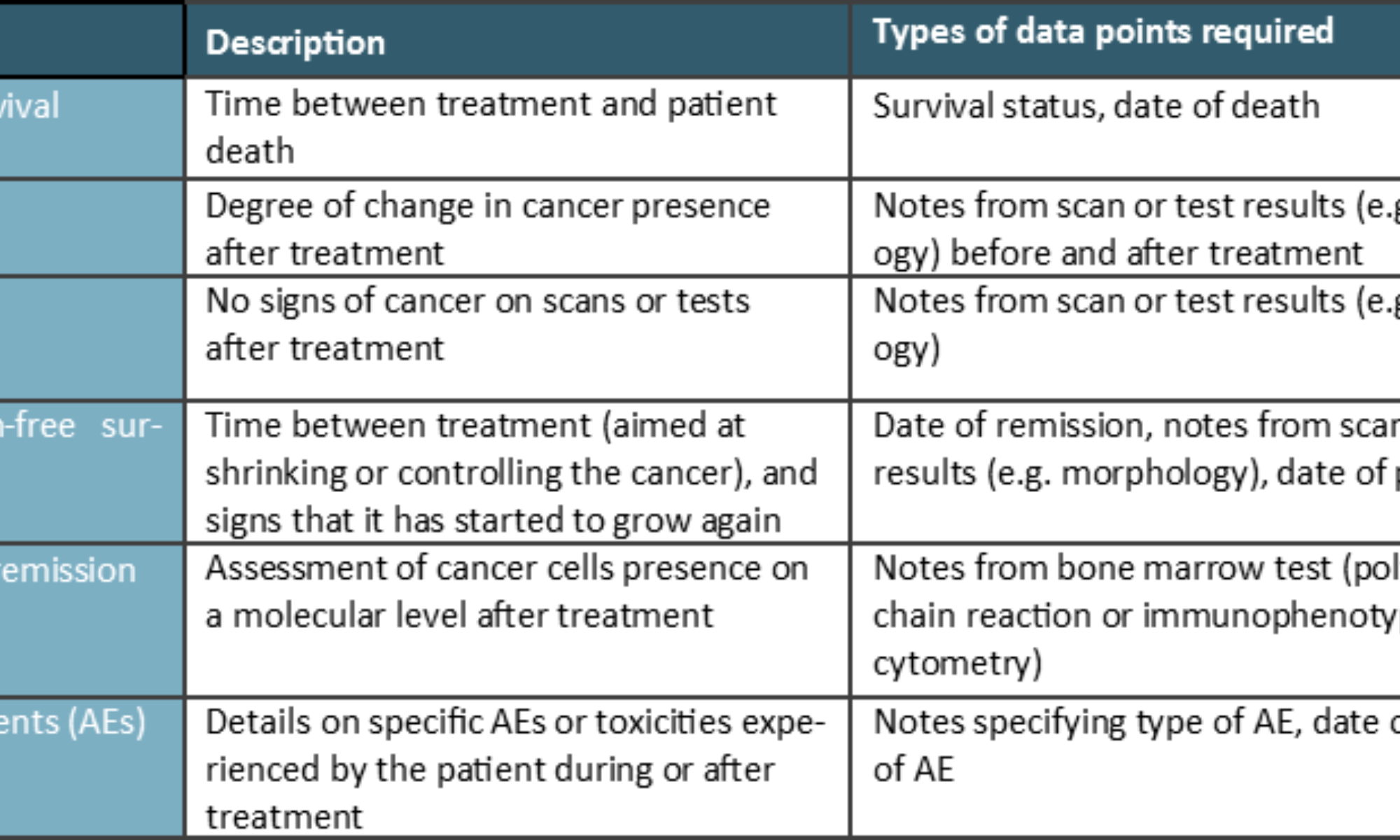
The gap analysis sought to establish the degree to which EBMT can capture clinical, economic and humanistic outcomes for the purposes of OBR. A key focus was clinical outcomes, as detailed in the table below.

We also considered economic outcomes, e.g. hospital admissions, and healthcare resource utilisation, as well as and humanistic, patient-reported experience or outcomes measures (PREMs or PROMs) such as quality of life (QoL) and patient satisfaction.
We applied secondary and primary research to explore these issues:
- Secondary (desk) research: An assessment of the guidance documents, data collection forms and data completeness reports available in the public domain
- Primary research: interview with EBMT experts to validate secondary research findings and to bridge information gaps
Findings
The EBMT maintains a registry encompassing all haematopoietic stem cell transplant (HSCT) procedures for all indications. It also stores data on immunosuppressive treatments for bone marrow failure syndromes (e.g. aplastic anaemias), and importantly also cell therapy treatments other than HSCT. The aim of the registry is to collect good quality clinical data, which are mainly used for research purposes, but which can also be used for other purposes, such as inspection, auditing and accreditation of transplant centres. Membership in the EBMT and reporting of data are voluntary, however, prompt reporting of transplant data is a core requirement for successful accreditation by the Joint Accreditation Committee of the International Society of Cellular Therapy (ISCT) and the EBMT (JACIE). JACIE accreditation is a (voluntary) certification that a transplant centre is performing to a required level of excellence using effective quality management systems. There are 53 transplant centres in the UK, all of them are members of the EBMT, and English centres are required by NHS England to be JACIE accredited in order to perform HSCTs. Trusts upload data to the EBMT registry on an annual basis, and in cases where individual patients have been seen more than once during that year, more than one data entry is submitted (e.g. for patients who are in the first year of treatment, hospitals would report data for both day zero and 100).
The EBMT has a host of European national counterparts, and The British Society of Blood and Marrow Transplantation (BSBMT) functions among other things as an interface between the EBMT and UK transplant centres on data issues. A small minority of transplant centres send their data to BSBMT for entering into the EBMT registry, however, the majority enter data directly into the EBMT registry. The BSBMT can then access that data, e.g. to undertake UK-specific analyses.
The EBMT comprises data collection forms relating to HSCT, and importantly also specific forms for cell therapies other than HSCT, e.g. CAR T-cell therapies. For HSCT patients, there are two types of forms, the Minimal Essential Data (MED)-A form, which is mandatory for all members to submit to retain full EBMT membership, and the MED-B form, which is optional and contains additional disease and HSCT-specific data. The development of the cell therapy-specific form stems from the EBMT’s long-standing interest in the use of cell therapies. This interest has, among others, seen EBMT involved in efforts undertaken by the European Medicines Agency (EMA) to explore how the registry might perform a future role in the execution of post-marketing data collection requirements commonly levied by the EMA for ATMPs. The EBMT established the Cell Therapy Registry with the aim to collect data on the administration and long-term follow-up of somatic cell therapy medicinal products and gene therapy medicinal products, including (but not limited to) CAR T-cell therapies, as well as data on the clinical characteristics and outcomes.
The cell therapy form includes sections for diagnosis, cell material type, cell manipulation, infusion episode(s), and outcomes like death, toxicities, best response after completed treatment (e.g. remission), complications, first relapse/progression, persistence of infused cells, and several disease area-specific sections. Data are to be collected at day zero, day 100, six months, 12 months, and annually thereafter.
The EBMT has actively pursued a broad application for the cell therapy form in Europe. In June 2018, the EMA’s Committee for Medicinal Products for Human Use (CHMP) published a draft qualification stating that it considers the cellular therapy module of the EBMT registry as an appropriate data source for post-authorisation studies to support regulatory decision making for CAR-T cell therapy used in haematological malignancies (a final qualification is expected by the end of 2019). Shortly after, the EBMT engaged with several manufacturers of gene therapies (including Novartis, bluebird bio, MolMed, Celgene, and Kite) to further develop the existing cell therapy form so it can be used across different ATMPs. The EBMT has a stated ambition for the future that the registry can be utilised also for HTA purposes, and anticipates to build further on discussions with the European Network for Health Technology Assessment (EUnetHTA).
As the revised EBMT Cell Therapy forms have only recently been introduced, there is no completeness data available for them
Clinical outcomes
The table below details the data capture and gap analysis based on the EBMT Cell Therapy Med-A Forms and user guide from March 2019. Overall, the EBMT Cell Therapy Med-A Form collects many of the clinical endpoints included in our gap analysis, however, economic and humanistic outcomes are lacking.
- Overall survival (OS) can be tracked as through the EBMT’s Cell Therapy form includes data fields for both date of treatment and date of death
- Response is tracked at every follow-up
- Remission and progression-free survival (PFS), both are tracked
- Molecular remission is detailed only at the time of treatment, however, this is not included in the forms for the post-treatment follow-ups, meaning it does not seem possible to track this outcome over time
- Toxicities/adverse events are tracked to a large extent, e.g. graft vs. host disease, cytokine storm, neurotoxicity, organ toxicity, bone marrow aplasia and other, in addition to secondary malignancies
Economic outcomes
EBMT does not capture economic outcomes like hospital admissions (inpatient or outpatient), the cost of the drugs or procedures involved, or any other detail on health resource utilisation beyond the dosages used. Costs and resource utilisation data is possible to collect through other sources, e.g. the Hospital Episode Statistics, or Secondary Uses Services using the NHS patient identification numbers, however, this requires investment in systems integration, as well as overcoming governance issues.
Humanistic outcomes
EBMT does not capture quality of life outcomes, whether disease-specific or generic (e.g. the EQ-5D, which is a central component of the cost-utility framework used in HTAs by NICE among others).
Implications
The cell therapy form currently used in the EBMT shows considerable potential to serve as a conduit for OBR, however, this would facilitate OBR schemes based on key clinical outcomes only, economic outcomes or PROMs/PREMs are not captured. Economic outcomes can potentially be sourced from Hospital Episode Statistics (HES), (Electronic) Health Records (EHR), SUS, and other sources using patients’ NHS ID numbers, however, this requires investment in systems integration, as well as overcoming governance issues (e.g., EHR data are under the governance of individual trusts). PROMs and PREMs such as the ability to return to normal daily activities are increasingly regarded as important, perhaps especially for younger patients, but there are currently no national databases to collect these data. Nor is there currently an agreed standard or consensus on which PROMs and PREMs are most relevant in cancer, meaning that efforts would need to be made to identify these as well as facilitating an infrastructure to capture the data.
The suitability of the EBMT cell therapy form for tracking patient outcomes can be illustrated by the EMA’s endorsement of this as a potential vehicle for implementing the regulatory requirements for ATMPs to collect data post launch. The initiatives to involve industry and importantly also physicians (the development of the EBMT forms is driven by physicians) should act to increase buy-in also from these stakeholders. Importantly, it is also scalable across the devolved nations of the UK and across Europe, meaning that it has the potential to become a larger-scale source of real-world data, which would be particularly valuable in rare and ultra-rare indications, which many cell and gene therapies in development are targeting. Furthermore, including additional data fields in the EBMT forms (e.g. economic and humanistic outcomes) would also make for a more comprehensive data source in one place.