The HE&MA function of the CGT Catapult engaged with an ATMP developer to identify the US price and access potential for a novel ATMP targeting a rare disease associated with an elderly population.
The objectives of the engagement were to:
- Detail the current and emerging reimbursement and funding (i.e. coverage) environment in the disease area and therapeutic position of interest in the US, with an emphasis on Medicare as the target patient population is ≥ 65 years of age
- Understand US payers’ view on the following:
- The positioning of the novel ATMP in the treatment algorithm
- The supporting data requirements that enable adoption
- Understand the reimbursed price potential and volume opportunity of the novel ATMP in the US
Assessing the price and volume opportunity
In order to undertake a meaningful analysis of pricing and reimbursement (P&R) potential at launch for the novel ATMP currently in development, it was important to leverage the methodological approaches that are expected to influence coverage decision-making for a highly innovative therapy in the future. To provide the most comprehensive advice possible, the HE&MA team applied a triangulation of methodologies to understand the price and volume opportunity and inform the commercial strategy.

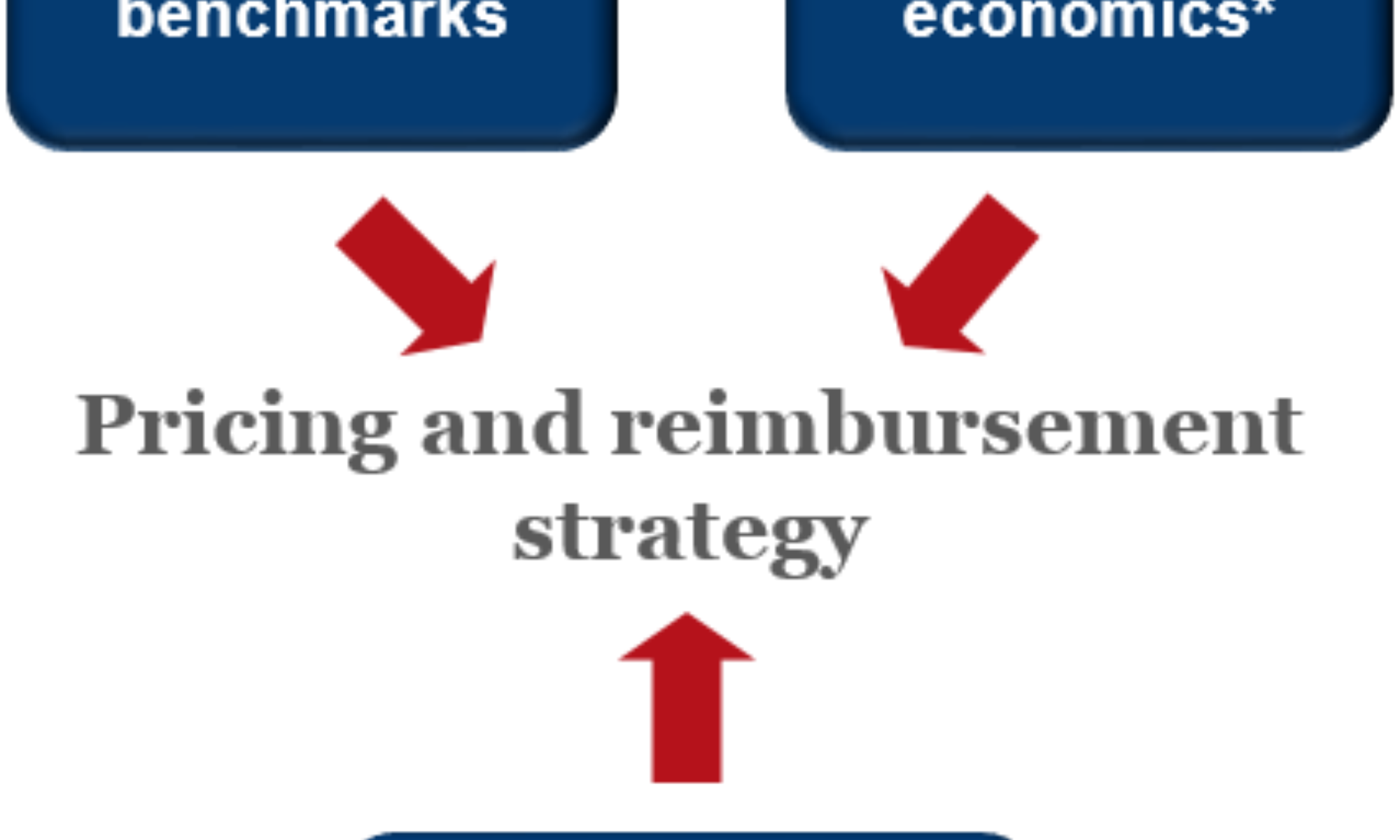
This triangulation allows us to draw on the learnings derived from secondary research on pricing benchmarks (including reimbursed price and associated restrictions for current therapeutic options as well potential impact from new market entrants), health economic analysis comparing the novel intervention against existing (cost-utility and budget impact analyses) as well as primary research with key market access stakeholders (payers and their clinical and economic advisors). The first two methodologies help inform the development of hypotheses around price and volume, which are subsequently tested through the third methodology (primary research).
Pricing benchmarks
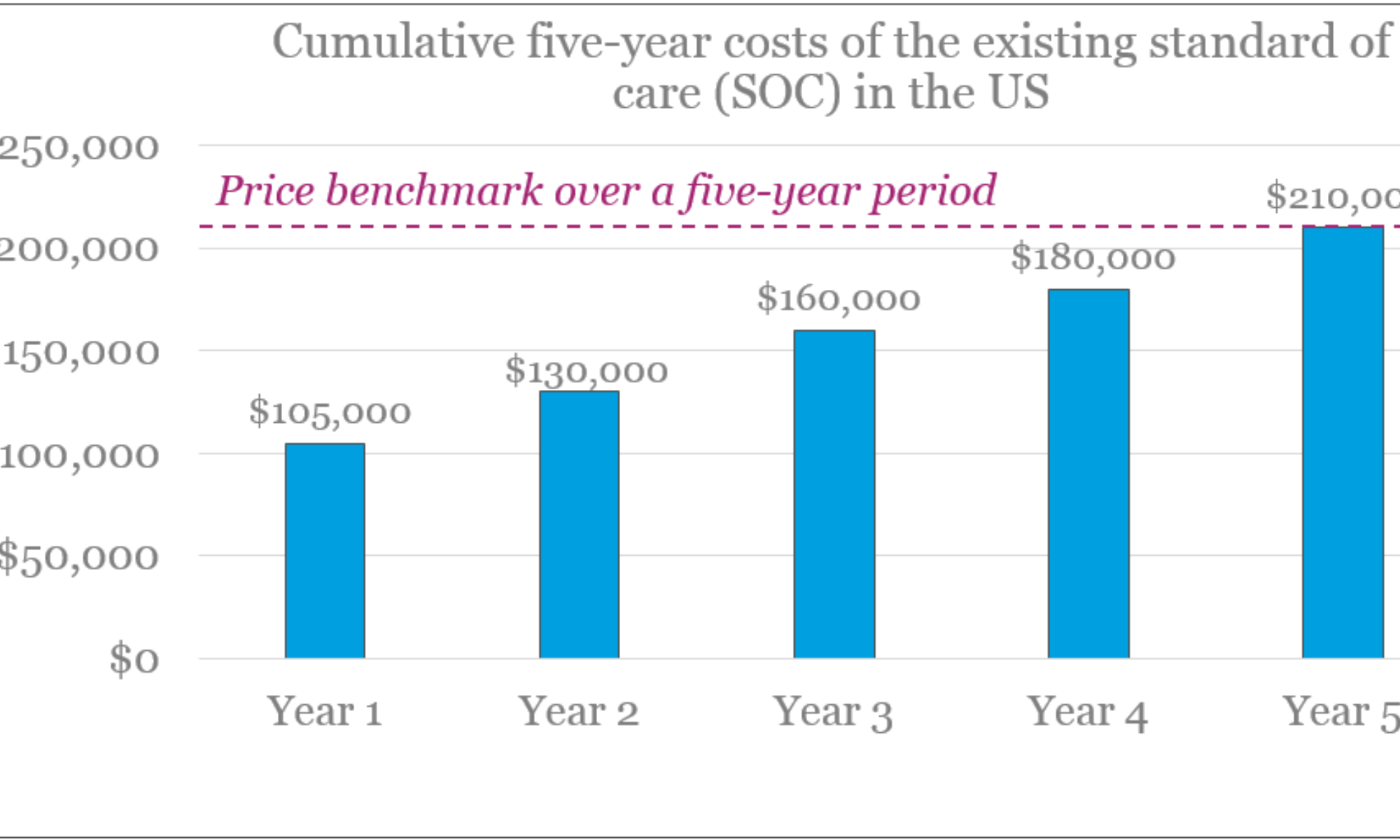
The starting point for the triangulation is the identification of the healthcare costs that the novel therapy aims to displace. As the novel ATMP is aiming to make value claims around displacing the need for the Standard of Care (SOC) over a five-year period (anticipated length of clinical data at launch substantiating claims of five-year sustainability of effect), we calculated healthcare costs with the SOC over the same period. The Medicare perspective was particularly pertinent in this project, given the elderly target patient population. Through desk research, we detailed Medicare’s coverage determinations and funding arrangements for the SOC in the target therapeutic position.
Health economics
Cost-utility analysis (CUA)
In the United States, CUAs have traditionally had little impact on coverage decisions, however recent developments indicate a shift in interest towards a greater use of such value-based approaches. The Institute for Clinical and Economic Review (ICER) has a clearly defined approach to CUA and uses the following ranges of willingness to pay (WTP) per additional QALY generated by the new therapy :
- <$50,000/QALY: High value; considered cost-effective
- $50,000-$175,000/QALY: Can be considered cost-effective and long-term value for money if ‘Contextual Considerations’ and ‘Other Benefits and Disadvantages’ exist (see below) that contribute to the long-term value
- >$175,000/QALY: Low value; not considered cost-effective
While the ‘Other benefits and disadvantages’ focus on the outcomes for the patient and caregivers, etc., the ‘Contextual Considerations’ focus more on disease burden, unmet need in the therapy area, and the uncertainty surrounding the long-term safety and efficacy. In ultra-rare indications (i.e. where the treatment is envisaged for a population of less than 10,000 US patients, or ~3/100,000), ICER’s value assessment framework allows the discretion to accept a higher cost per additional QALY than $175,000, and gives greater weight to ‘Other Benefits’ and ‘Contextual Considerations’.
Based on these considerations, we undertook the below steps to conduct the CUA:
- Perform a pragmatic evidence review of the published literature to:
- Detail the clinical and economic outcomes associated with current SOC
- Estimate the healthcare resource utilisation pertaining to the SOC
- Identify relevant health economic analyses to inform the model structure
- Build a Markov state-transitioning model featuring two arms: one for the SOC, and one for the novel ATMP, in order to compare the costs and outcomes (QALYs) accrued in the two arms over patients’ remaining lifetime
- The model was structured according to health states defined by patients’ underlying disease severity and sub-states for their level of symptom control, reflecting the disease trajectory for the target patient population
- The model was populated with costs, outcomes, transition probabilities and mortality from the published literature
- Identify the health-economically justified price potential, based on reaching, but not exceeding, the relevant WTP/QALY, in two efficacy scenarios:
- Patients treated with the ATMP achieved an improved symptomatic control
- Patients improved both in terms of symptoms and their underlying disease (i.e. disease modification)
The results of the CUA for the two efficacy scenarios are displayed in the figure below and compared to the results of the price benchmark analysis for the SOC.
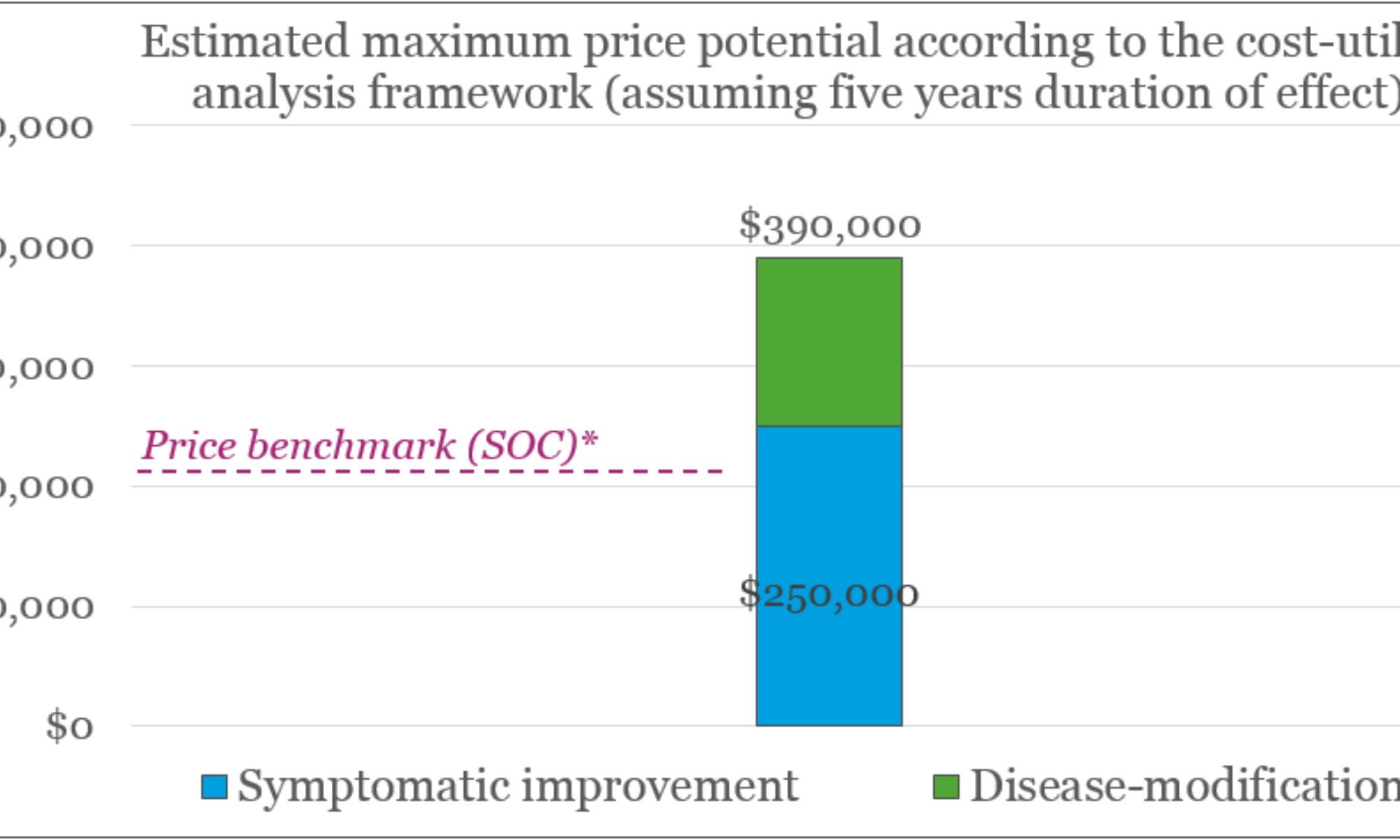
These results show that in the scenario where the ATMP achieves a symptomatic improvement alone, the price uplift provided by the CUA is somewhat modest as compared to the price benchmark (from $210k up to $250k). In the disease-modifying scenario, the value potential is much greater (up to $390k), driven mainly by greater QALY gains.
Budget impact analysis (BIA)
The BIA is a health economic assessment of affordability that helps decision-makers establish whether the increase in spending from adopting the new therapy is acceptable, or whether price or volume concessions are necessary to manage the healthcare budget. Our BIA was undertaken based on the results of the price benchmarking and the price points found in the CUA. The BIA explored the budget impact in year one according to the two efficacy scenarios tested in the CUA (i.e. symptomatic improvement and disease modification) using two reimbursement scenarios: first where a full upfront price is charged for the ATMP at the time of administration to patient, and second where performance-based annuity payments are used to spread the product cost over five annual installments (i.e. the period over which the therapy is making efficacy claims), and conditional upon maintenance of therapeutic effect. Our BIA had two main objectives:
- To inform the primary research discussions with budget holders, to facilitate materials for them to react to when discussing potential access restrictions
- To test the potential volume implications of the budget impact threshold proposed by ICER in 2017 of $457.5 million (for 2017) for annual net budget impact per drug
The results of the BIA showed that a full upfront payment would result in a considerable budget impact in both efficacy scenarios, while an annuity-based payment scheme would in fact result in cost savings in year one. If the budget impact threshold proposed by ICER was to be implemented, it might pose a substantial limitation to the target patient population if a full upfront payment is charged at the time of administration, while the annuity-payment scheme would mean there would be no limitation on patient numbers.
Primary research: advisory board validation
The final step of our research was an in-depth testing of the results from the pricing benchmark and the health economic analyses. We used these findings, as well as our expertise in the market access drivers and processes in the US, to build hypotheses around the price and access potential for the novel ATMP. These hypotheses were then tested in a full-day advisory board with key market access stakeholders. The participants in the advisory board included two key opinion leader clinicians and six payers who are ‘price-sensitive’ customers who have influence over reimbursement decisions, funding, and product evaluations.
Central to the preparation for the advisory board is the development of the discussion materials to ensure that the discussion had a logical flow and captured the insights needed to complete the analysis including:
- Current treatment landscape: existing SOC, clinical and economic outcomes, emerging landscape and unmet need
- Assessment of the target product profile of the novel ATMP: strengths/weaknesses, likely therapeutic position
- Price and volume assessment for the two efficacy scenarios
- Informed by the Gabor Granger methodology, i.e. understanding the relationship between different price points and the implications for volume
- Evidence requirements to substantiate the target value proposition; impact on price and volume opportunity
- Funding and access considerations
Research findings
The key findings in terms of reimbursed price potential for the novel ATMP in the US as informed by our methodology triangulation are summarised in the figure below:
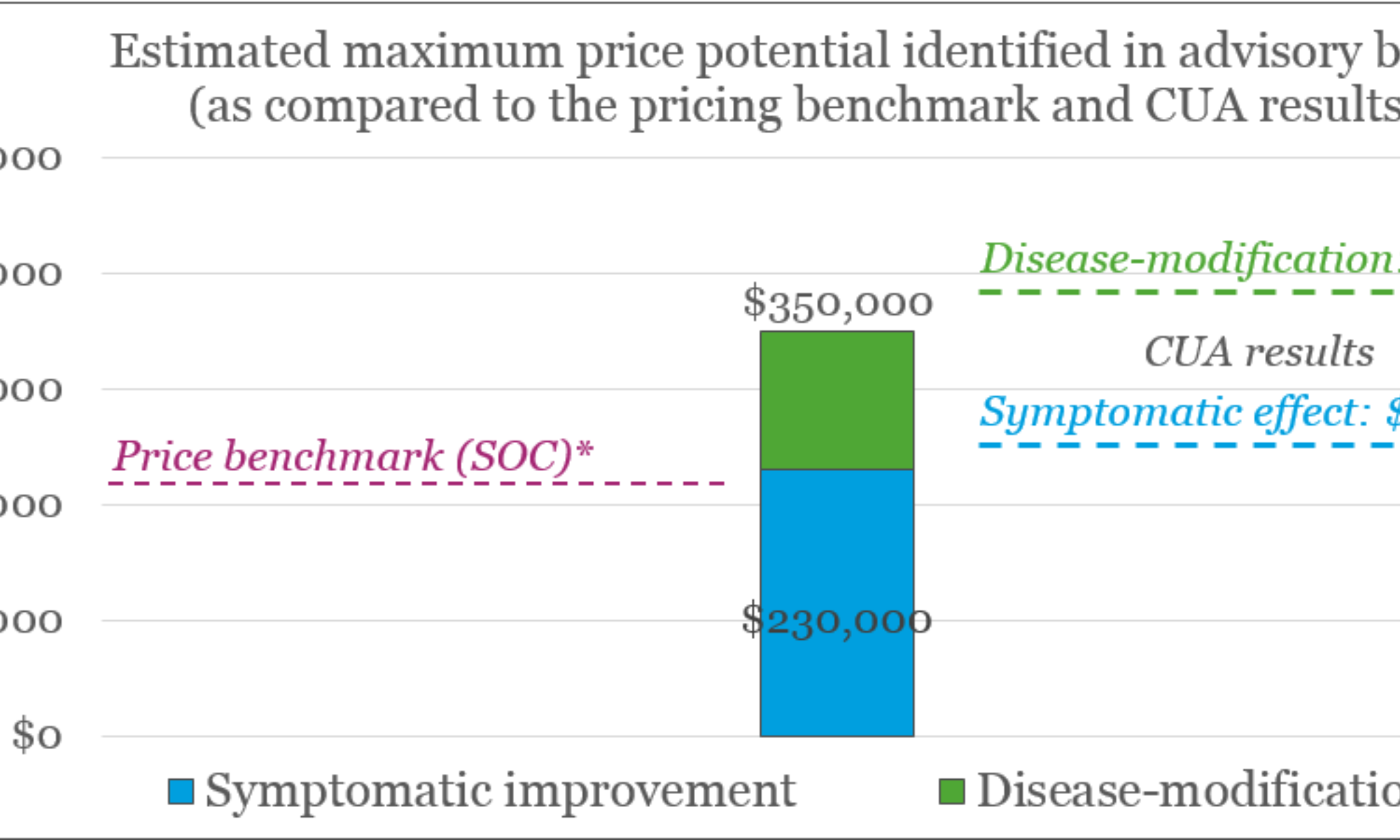
Subsequently, we detailed the access and volume implications of these price levels, including likely market shares in first five years post-launch, as well as strategies to minimise adoption risk
Conclusions and recommendations: The added value of the CGT Catapult
The US market is complex, and developing a commercial strategy that optimises the chance of commercial success requires a detailed understanding of the challenges and opportunities within it. The HE&MA team of the CGT Catapult uses its in-depth healthcare system expertise and extensive experience in P&R of high-cost, innovative ATMPs to guide the transition from the desk research to primary research in order to facilitate the most meaningful and relevant insights from the key market access stakeholders.
The final step of the project is using the insights gained through desk research and primary research to formulate conclusions and recommendations to help shape the commercial strategy. These enabled the developer of the novel ATMP to understand:
- The value-maximising therapeutic positioning, informed by the unmet need, room for innovation and impact on price and volume
- The key clinical and economic value drivers to be included in the Target Product Profile and evidence generation plan
- The inter-relationship between incremental benefit, supporting evidence, reimbursed price potential, manufacturing costs and profit margins, in order to:
- Define product performance and manufacturing cost thresholds for commercial viability
- Inform clinical and manufacturing strategy accordingly
- Forecast how different efficacy and evidence levels impact revenue potential and profitability
- The key P&R and market access hurdles and risk-mitigating strategies that:
- Enable reimbursement at a commercially viable price in the revenue-maximising target population
- Optimise the market share at launch and over time
By clearly identifying the relationship between different levels of product performance and commercial viability, our analysis allowed the developer to define ‘go/no-go’ decision-making criteria reflecting threshold levels for efficacy and manufacturing costs. Furthermore, our work provided an outline for an early pricing and reimbursement strategy for the US informed by the hurdles and risk mitigation strategies identified. This forms the basis for the ongoing process of fine-tuning the developer’s vision for the positioning, pricing and reimbursement potential, evidence generation activities and market access strategies as the novel ATMP reaches a more mature development stage. Also, our scenario analysis including projections of revenue and profitability enabled the developer to confidently adjust their financial forecasting, both for internal use purposes and for use in engaging with investors.