While cell and gene therapies have substantial therapeutic potential, they are costly to research, develop, manufacture and deliver, which necessitates a high price in order to be commercially viable.
The combination of great therapeutic potential and high prices has led to increased consideration of performance-based reimbursement (PBR) schemes in order to facilitate patient access at a price that reflects the therapeutic benefit the product delivers in the real world.
The Health Economics and Market Access function at the Cell and Gene Therapy Catapult has published a series of peer-reviewed articles on topic of reimbursement and performance-based schemes specifically, and we argue that two key things need to be in place in order for such schemes to work:
- An appropriate data collection infrastructure (e.g. registry) for collecting clinical and/or economic outcomes
- A clinical practice that ensures that the necessary data is captured and entered into the database or registry
In previous work, we have undertaken a top-level assessment of the existing data collection infrastructure in the therapy areas most likely to see launches of cell or gene therapies over the next five years. In that article, we show how thalassaemia, on the face of it, is a therapy area where the available registry, and patient follow-up in clinical practice seems conducive to adopting a PBR scheme. Given the likely imminent launch of gene therapies in the thalassaemia area, we wanted to have a closer look at the appropriateness of the data collection in this therapy area, and we expand on this here.
The objective
The objective of this exercise is to detail how data collection works in clinical practice in thalassaemia, more specifically through the National Haemoglobinoapthy Registry (NHR), and to explore the extent to which this could potentially facilitate PBR for gene therapies.
The deliverable – research methods and findings
Methods
We applied secondary and primary research to explore this issue:
- Secondary (desk) research: An assessment of the data captured by the NHR, and whether these include outcomes that could facilitate performance-based reimbursement
- Primary research: interview with a key member of the NHR steering committee to validate secondary research findings and to bridge information gaps
Current use of the NHR
The National Haemoglobinopathy Registry (NHR) includes patients with red cell disorders (mainly sickle cell disease and thalassaemia major) living in the UK, and collects data from haemoglobinopathy centres, as required by the Department of Health. Our assessment of the NHR revealed some interesting overall observations:
- Since its inception in 2009, the proportion of thalassaemia patients registered with the NHR has increased considerably, from around 900 in 2009, to 1,327 by January 2019
- While the aim is for every thalassaemia patient in the UK to be entered into the registry, and have their data captured regularly, this is not the case
- An estimated 80% of the 49 centres that treat thalassaemia patients upload data to the NHR
- A key reasons for the ~20% shortfall is thought to be a lack of administrative staff resource (e.g. data managers) to comply with the manual data entry into the registry
- The data completeness rate for patients on the registry is good, and thought to be around 90%
Key data captured in the NHR is detailed in Table 1 below.

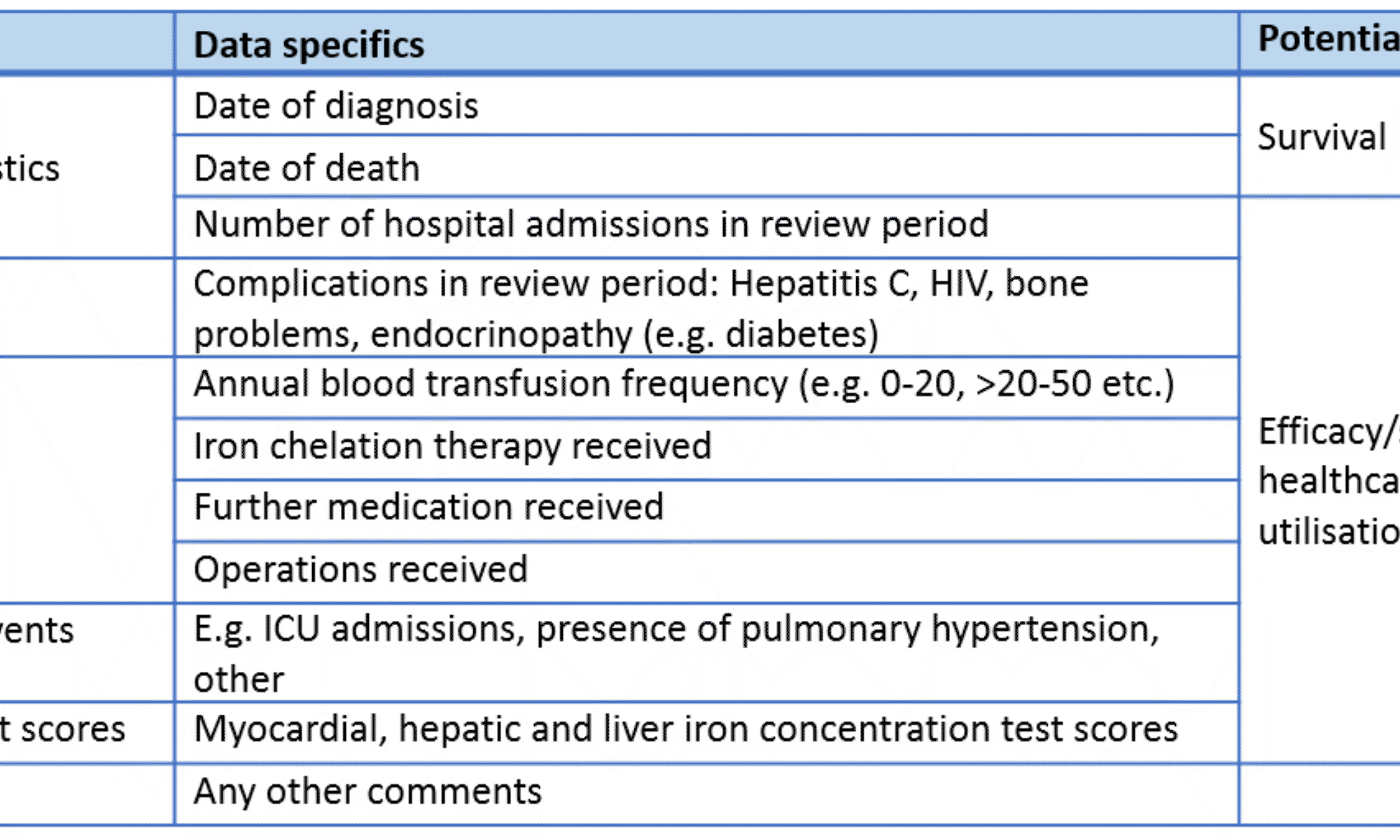
Based on the data fields included in the NHR, there is reason to believe that the NHR could perform a function as a data collection infrastructure for PBR in thalassaemia. In particular, the data on the annual blood transfusion frequency is a key proxy outcome for therapy efficacy, as it would be low or zero if the patient’s production of red blood cells has been effectively restored. Similarly, the use of iron chelation therapy is another key proxy outcome as this signifies the presence of iron overload in patients, which is a central side effect of blood transfusion and therefore a therapeutic focal point.
However, there are several data points that would be useful for PBR that are not present in the NHR in its current form, e.g.:
- Blood haemoglobin levels (proxy for anaemia) – Treatment efficacy proxy
- Outcomes relating to patients undergoing haematopoietic stem cell transplantation (HSCT), which is the only current cure for thalassaemia
- Infection-related complications beyond HIV and hepatitis C
- Units of blood transfused (this is captured in the electronic patient record); NHR only records the transfusion frequency
Although the NHR collects many data points that could be useful for facilitating PBR, there are certain structural features of the NHR that limit its applicability. Firstly, reporting into the NHR is done on an annual basis (as patients are routinely seen annually), meaning that shorter time-interval reimbursement schemes would be challenging to run through the NHR. Secondly, the NHR is comprised of a large number of binary data fields, which limits the quality and detail of data the capture. Thirdly, there is a lack of official reporting, tracking and analysis of data completion / quality, which means it is hard to tell e.g. what the actual completion rates are, despite a push to improve this through the Commissioning for Quality and Innovation (CQUIN) initiative from 2016.
Importantly, the NHR does not capture data specific to HSCT, and this would likely extend also to patients undergoing gene therapies that require haemodepletion, which is the case for some of the thalassaemia gene therapies nearing market. The European Bone Marrow Transplant (EBMT) registry is being considered as a potential avenue for such patients, however, this is still to be determined.
Furthermore, a key challenge to overcome in order to optimise the NHR for reimbursement purposes is around staff resource shortages. The thalassaemia service faces increasing patient numbers, and an ageing workforce, which means that additional resource is needed to ensure compliance with data capture. E.g. there are currently fewer than 12 full time equivalents of adult patient consultants providing care in England (nine paediatric patient consultants), and 30% of specialised nurses are set to retire over the next five years. Additionally, there are reports of patients being reluctant to share their data into the NHR, which is highlighted also by NHS England as a barrier to enabling a national registry providing effective support to clinical management. This may go some way in explaining that only an estimated 80% of centres are uploading data to the NHR.
Future developments
NHS England has recognised the challenges faced by the haemoglobinopathy services, and are driving a review of how these are organised and paid for, to improve services for thalassaemia patients. Their proposed solution includes the following key points:
- Up to 10 Haemoglobinopathy Coordinating Centres (HCCs), funded to provide network development/ leadership and learning/ education (this will be commissioned through a procurement exercise), with responsibility (among other things) for ensuring that NHR data is submitted by organisations within the network
- Circa 24 Specialist Haemoglobinopathy Teams (SHT), which will be funded to undertake specialist clinical activity; their funding will in part be tied to compliance with entering data into the NHR
- A National Haemoglobinopathy Panel, with membership drawn from the HCCs, will provide advice on novel treatments and options for individuals with complex needs; this panel will assess particularly complex patient cases and decide on referral for treatment modalities such as HSCT and gene therapies
- The National Haemoglobinopathy Registry is being cleaned up and revised in order to make it more user friendly and improve its functionality; in the future, funding will be linked to compliance with entering NHR data
- Funding for thalassaemia services will change towards a “year of care” tariff for clinical care in 2021, but this is unlikely to affect high cost items such as HSCT and gene therapies, which are (likely) paid for separately
Implications
Although the available data collection infrastructure and practice is relatively good in thalassaemia, as compared to many other therapy areas, it needs to be improved in order to facilitate PBR. More specifically, the NHR in its current form only partially provides the framework needed to enable PBR in thalassaemia. If appropriate staff resource is provided and there is a successful drive towards ensuring all patients have their data recorded in the NHR, it may be possible to implement a PBR scheme in thalassaemia on the cohort-level, based on the annual reviews. There is a push from NHS England towards improving compliance with NHR, which is encouraging, however, this may not be sufficient to tackle the challenge of patients opting not to share their data.
The NHR is unlikely to provide the appropriate infrastructure for implementing patient-level reimbursement schemes, or schemes that require more frequent than yearly readings, as patients are only reviewed and have their data collected annually. Patient-level reimbursement schemes would likely only be possible by approaching each trust individually (as the trusts own the data) and secure access to individual patient data, however, this is a highly fragmented effort, and may not be successful in accessing all relevant patients.
The EBMT can potentially be a relevant registry for gene therapies that require haemodepletion. Patients on the EBMT have data recorded at day 100, and annually thereafter, and UK providers’ compliance with entering data into the EBMT is 100%. There is also a drive to include patients undergoing gene therapies requiring haemodepletion into the EBMT, meaning it is a potential source of outcomes data. Despite the potential for using EBMT in gene therapy patients, it the NHR might still play a role also for these patients, as long as they continue to have their annual thalassaemia appointments.
Importantly, a central challenge to facilitating PBR in thalassaemia is overcoming the staff resource shortage, which is a barrier to data collection. Implementing such reimbursement schemes is reliant on NHS England’s restructuring efforts being successful in increasing compliance with the NHR and improving patient trust so that opting out of the NHR is minimised.