Outcomes-based reimbursement, whereby the financial remuneration for a therapy is made conditional on achieving and/or sustaining certain patient outcomes, is an often considered means to manage the introduction of high-value therapies. This approach can be particularly useful for one-off cell or gene therapies that have the potential to deliver long-term health improvements, but where the clinical data provided at launch falls short of robustly demonstrating the long-term benefit to NHS decision-makers.
In the regenerative medicines study from 2016, The National Institute for Health and Care Excellence considered an outcomes-based reimbursement scheme whereby a one-off therapy was paid for like a chronic treatment, or “…for each period of time that the health [benefit] is delivered at the individual patient level. That is, if the observed effectiveness in clinical practice was equal to the expected effectiveness, the manufacturer would receive the full value of the technology over the agreed period. However, if observed effectiveness was less than expected, payment would stop and the risk to the health system of over-payment would be limited.”
This means that payments for a one-off therapy would be staged over time, and that the NHS would only be liable to pay if the pre-agreed patient health outcome materialises and is sustained. There are several important and beneficial implications to this approach:
- Reducing the uncertainty around the cost-effectiveness of the therapy, which is one of the central factors affecting NICE’s recommendation for reimbursement in the NHS
- Reducing the financial uncertainty and risk for overpayment in case the product does not perform as expected in the real world
- Reducing budget impact at launch, which improves affordability (short-term)
- Can accelerate patient access to therapeutic innovation
- Rewarding and incentivising therapeutic innovation that provides health improvements in the real-world setting
Despite being a conceptually fairly simple idea, an outcome-based reimbursement scheme like the staged payment approach considered by NICE can only function properly if it is rooted in a data collection practice and infrastructure that provides the appropriate framework for such schemes.
The objective
In previous work, we showed that in oncology, there is a requirement to follow-up patients routinely and collect their data into the Systemic Anti-Cancer Treatment (SACT) database, meaning that an infrastructure is already in place that could potentially support the adoption of an outcomes-based reimbursement scheme. However, the question remains what the situation is in the other therapy areas that are likely to see launches of cell and gene therapies in the coming years.
The objective of this research is therefore two-fold:
- To provide a top-level scan for the indications most likely to see a launch of a cell or gene therapy (ATMP) in the UK over the next five years, and
- To perform a qualitative assessment of what (if any) data collection infrastructure and practice is in place in the UK in the relevant indications, and to provide directional insights on how conducive the current environment is for facilitating the adoption of an outcomes-based reimbursement scheme
The deliverable – research methods and findings
The indications most likely to see launch of cell or gene therapies in the UK in next five years
In order to identify the indications most likely to see a launch of cell or gene therapies in the UK in the next five years, we identified the cell or gene therapies at a mature development stage, i.e. Phase III clinical trial (or in registrational trial stage where this is identifiable1) with EU and/or US trial sites. Subsequently, we recorded the target indications for the products/trials identified.
Key sources included data from the Alliance for Regenerative Medicine (ARM) detailing the global Phase III cell and gene therapy trials (as used in their Quarterly Data Reports), the European Clinical Trial Registry, the Advanced Therapies Investment Report 2017 from Phacilitate, the horizon scanning services provided by the UK Medicines Information (UKMi) and the UK Innovation Observatory and a review of company pipelines online.
Table 1 details our research findings in terms of the indications most likely to see a cell or gene therapy launch in the next five years: A total of 58 therapies/trials, across 47 target indications in 12 therapy areas.

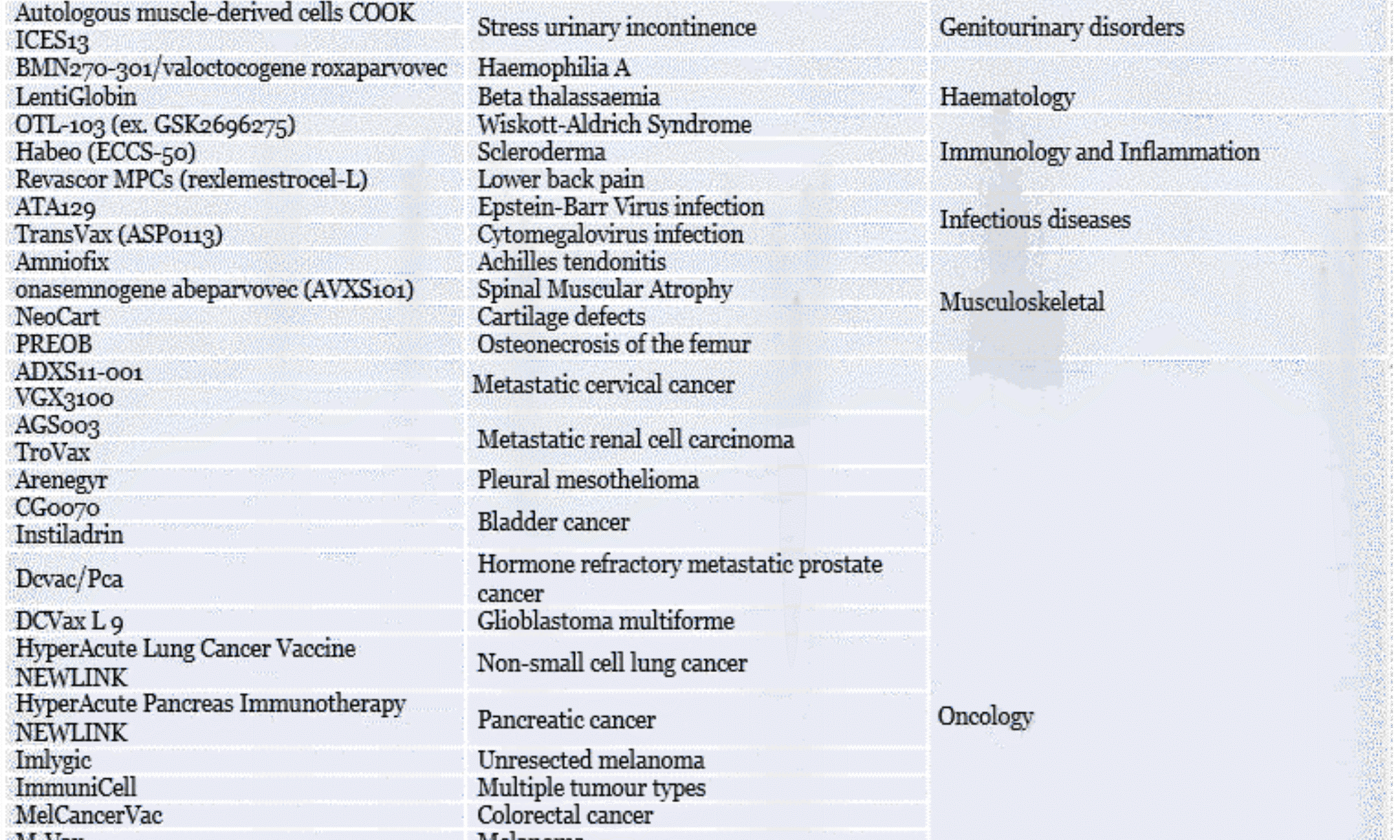
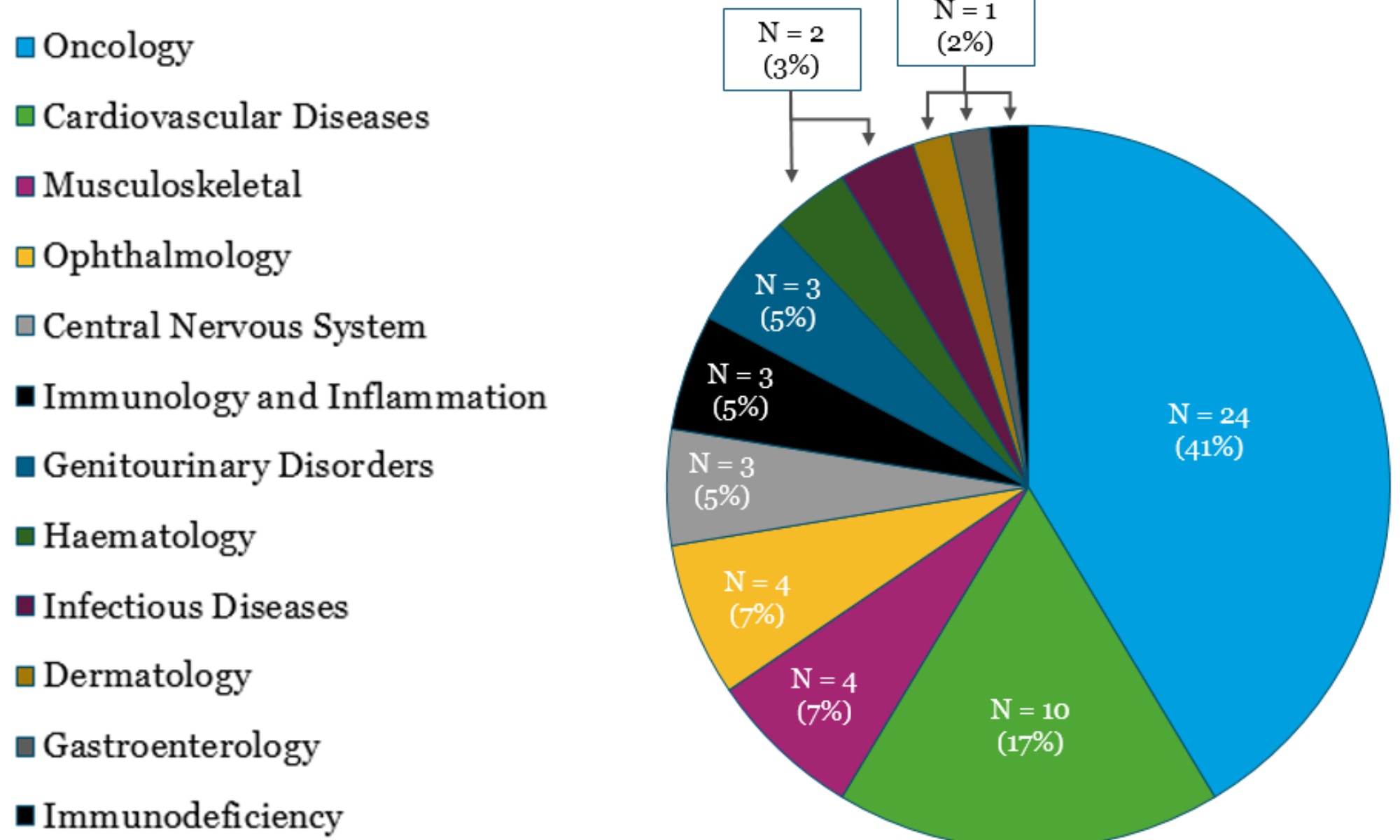
Figure 1 shows the number and proportion of cell and gene therapies in Phase III trials with EU and/or US trial sites according to therapy area. Our findings show that oncology is the therapy area has the highest likelihood to see UK launches of cell or gene therapies in the next five years, representing 40% of the therapies identified. Cardiovascular disease comes second with 10 therapies in development, representing three indications, while the remaining therapy areas have four or fewer therapies in development.
The existing UK data collection infrastructure and practice in the indications of interest
We applied a combination of secondary and primary research to determine what data collection infrastructure exists in the target indications of interest UK, and how it is used in routine practice.
- Secondary research: Internet searches to identify potentially relevant UK registries and databases in the indications identified
- Primary research: Structured interviews with key opinion leader (KOLs) clinicians in the different target indications to test our secondary research findings, and to explore the extent to which the existing infrastructures (if any) and clinical practice can facilitate long-term data collection for the purposes of enabling performance-based reimbursement
Figure 2 provides a graphical and numerical representation of our results, while Table 2 summarises the key findings of our secondary research and KOL interviews per indication.
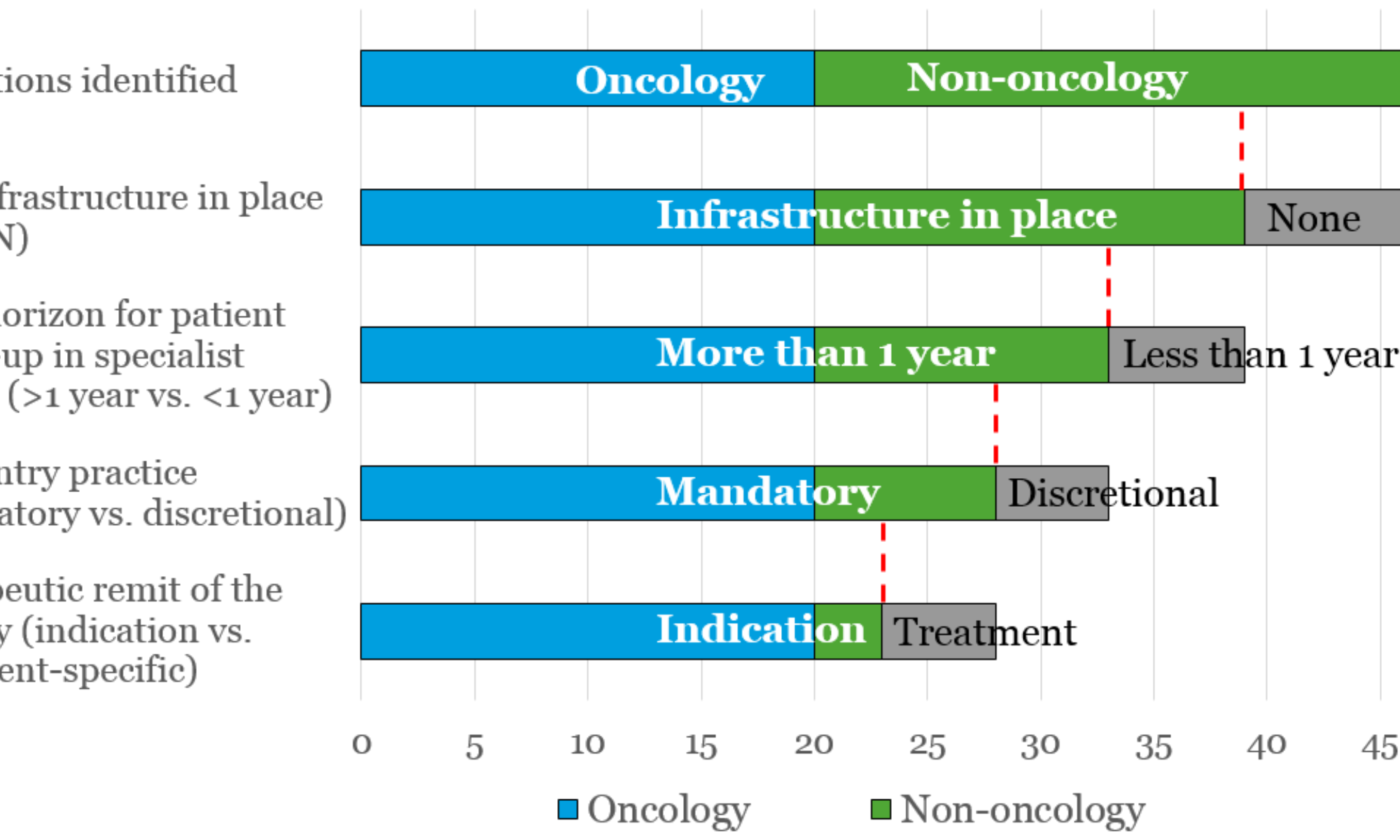
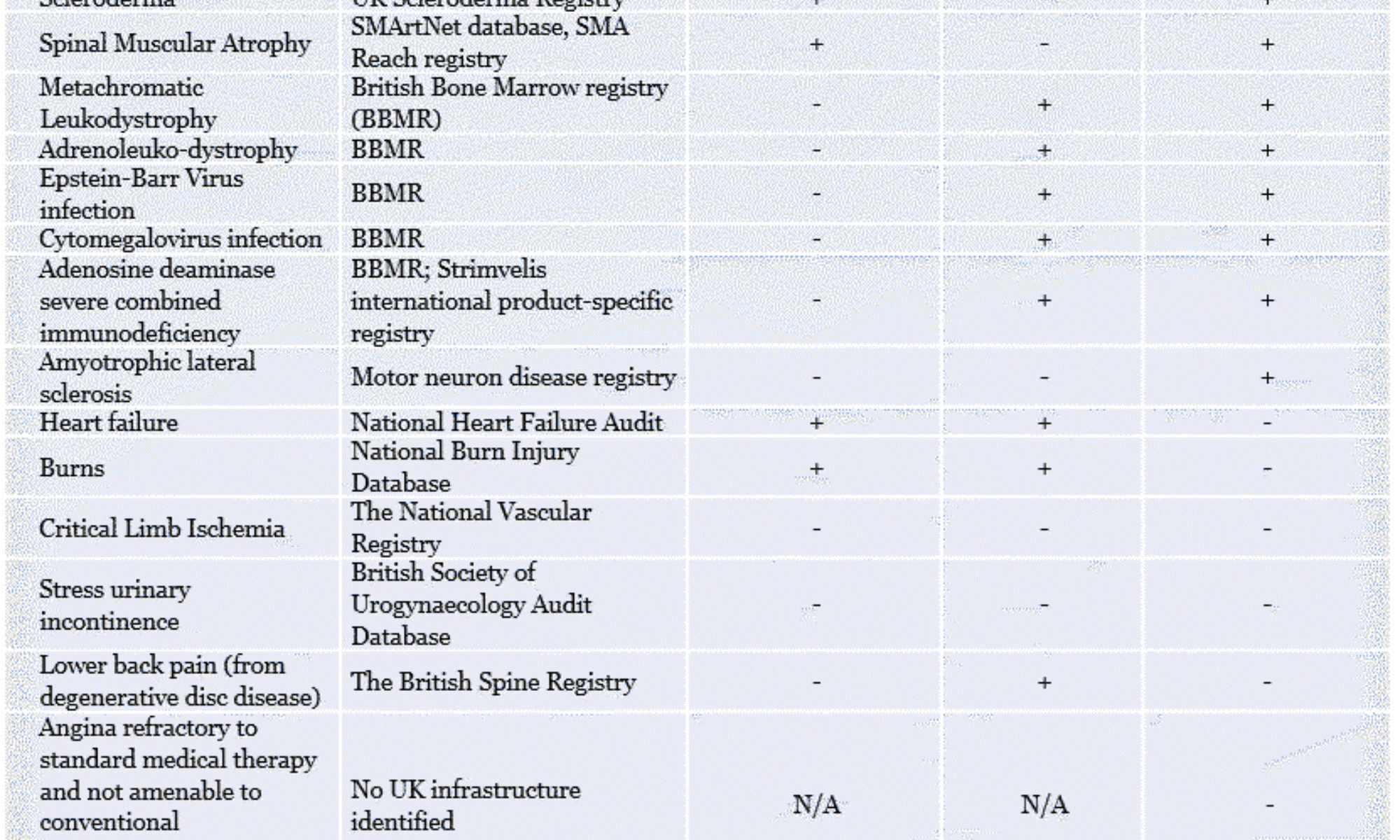
Table 2: Data collection infrastructure and current practice in the target indications of interest
* + indicates mandatory data entry; - indicates discretional data entry
** + indicates a follow up time >1 year; - indicates a follow up time <1 year
^ + indicates the registry is specific to the indication; - indicates the registry is specific to the therapy provided
N/A = not applicable
Our findings show that oncology (with its 20 indications), end-stage renal disease, haemophilia A and beta thalassaemia are the indications where a national data collection infrastructure is currently in place, and where patient follow-up and data collection is mandatory in the specialist setting beyond the one-year mark (in the latter three indications this is done indefinitely). These are the indications where the existing data collection infrastructure and clinical practice come closest be able to facilitate outcomes-based reimbursement schemes. But even in these indications upgrading is needed to enable the reimbursement mechanism and link all relevant stakeholders (clinicians, hospital pharmacists, finance, commissioners) while providing visibility for manufacturers and while maintaining patient confidentiality.
Among the remaining target indications, our results show that the majority have a data collection infrastructure in place, however, there are considerable differences between indications in terms of whether patients typically are followed up for more than one year, and whether data collection is mandatory.
More broadly, our interviews with clinicians revealed that patients with chronic and severe conditions tend to be seen routinely and sometimes indefinitely in the specialist setting, where data collection and monitoring is engrained in routine clinical practice. Since longer-term data collection in the specialist setting is part of the current clinical practice for such indications, the barriers to implementing outcomes-based reimbursement seem relatively modest if the appropriate data collection infrastructure were in place. Conversely, patients with conditions that are acute or require only short-term follow-up in the specialist setting (e.g. burns) are typically discharged into the primary care setting once they are stabilised, where long-term data collection is thought to be highly challenging.
Although our findings show that in many indications, the current clinical practice would have to change to enable longer-term patient data collection, it is important to highlight that the introduction of a cell or gene therapy would likely require the clinical pathway to change considerably anyway. Recent marketing authorisations granted by the EMA demonstrate that many cell or gene therapies are required to follow patients for more than a decade to document the long-term safety and efficacy. This means that while the current clinical practice in certain indications may be to discharge patients into the primary care setting, the introduction of a cell or gene therapy would likely require patients to be followed up in the specialist setting longer-term to collect patient data. This presents an opportunity to align the post-launch evidence generation for regulatory and reimbursement purposes, which is increasingly recognised by industry as well as regulators, payers, and HTA bodies.
This opportunity has been seized upon e.g. in Italy where The Italian Medicines Agency (AIFA) established a universal registry that serves both regulatory and reimbursement purposes, and which makes it possible to link prescriptions and payments/rebates to clinical criteria and outcomes.
The implication
The existing UK data collection infrastructure in the indications most likely to see launches of cell and gene therapies over the next five years needs upgrading to facilitate outcomes-based reimbursement such as the staged payment scheme considered by NICE.
In order to facilitate such reimbursement schemes, it is necessary to understand whether it is more useful to build on and integrate existing structures or to create a universal registry structure like the one operated by AIFA in Italy. Our recommendation is to undertake a detailed assessment of existing infrastructures in key therapy areas such as oncology, followed by a gap analysis to explore the costs and resource requirements associated with the two strategy options.
Regardless of the strategy chosen, an improved data collection infrastructure would be a key component in ensuring not only timely patient access, but also a better understanding and recognition of the value for the NHS, as well as an appropriate reward to manufacturers for innovation.
[1]Some cell and gene therapies aim for early or accelerated access using e.g. Phase II trial data where the unmet need and therapeutic potential is high
[2]The British Bone Marrow Transplant registry is also used for a subset of thalassaemia patients who undergo this type of treatment
Link to full article here