In previous work, we have shown that outcomes-based reimbursement (OBR), whereby payments to manufacturers are made conditional on achieving and/or sustaining a certain level of patient benefit, can reduce decision uncertainty and accelerate patient access to cell and gene therapies.
The administrative burden of such schemes are often cited as a reason why they are rarely applied in practice, and a central component of this administrative burden relates to the collection of outcomes data. We argue that there are two important factors that need to be in place in order for OBR schemes to be implemented, and both contribute to this administrative burden:
- An appropriate data collection infrastructure (e.g. registry) for collecting outcomes
- A clinical practice that ensures the necessary data is captured and entered into the database or registry
In January 2019, we published a peer-reviewed article detailing a top-level assessment of the existing data collection infrastructure in the therapy areas most likely to see launches of cell or gene therapies over the next five years. We found that oncology is by far the therapy area with the greatest number of cell and gene therapies at the pivotal trial stage, and that the Systemic Anti-Cancer Therapy (SACT) dataset seems like a promising framework for potentially facilitating OBR in oncology.=
The objective
Given the potential benefits of OBR, and the strong pipeline of gene therapies in oncology, we wanted to have a closer look at the SACT dataset. The objective of this exercise is therefore to perform a gap analysis of the SACT dataset to determine its use in practice, and its applicability for facilitating OBR in oncology in England.
The deliverable – research methods and findings
Methods
The gap analysis sought to establish the degree to which SACT can capture clinical, economic and humanistic outcomes for the purposes of OBR. A key focus was clinical outcomes, as detailed in the table below.

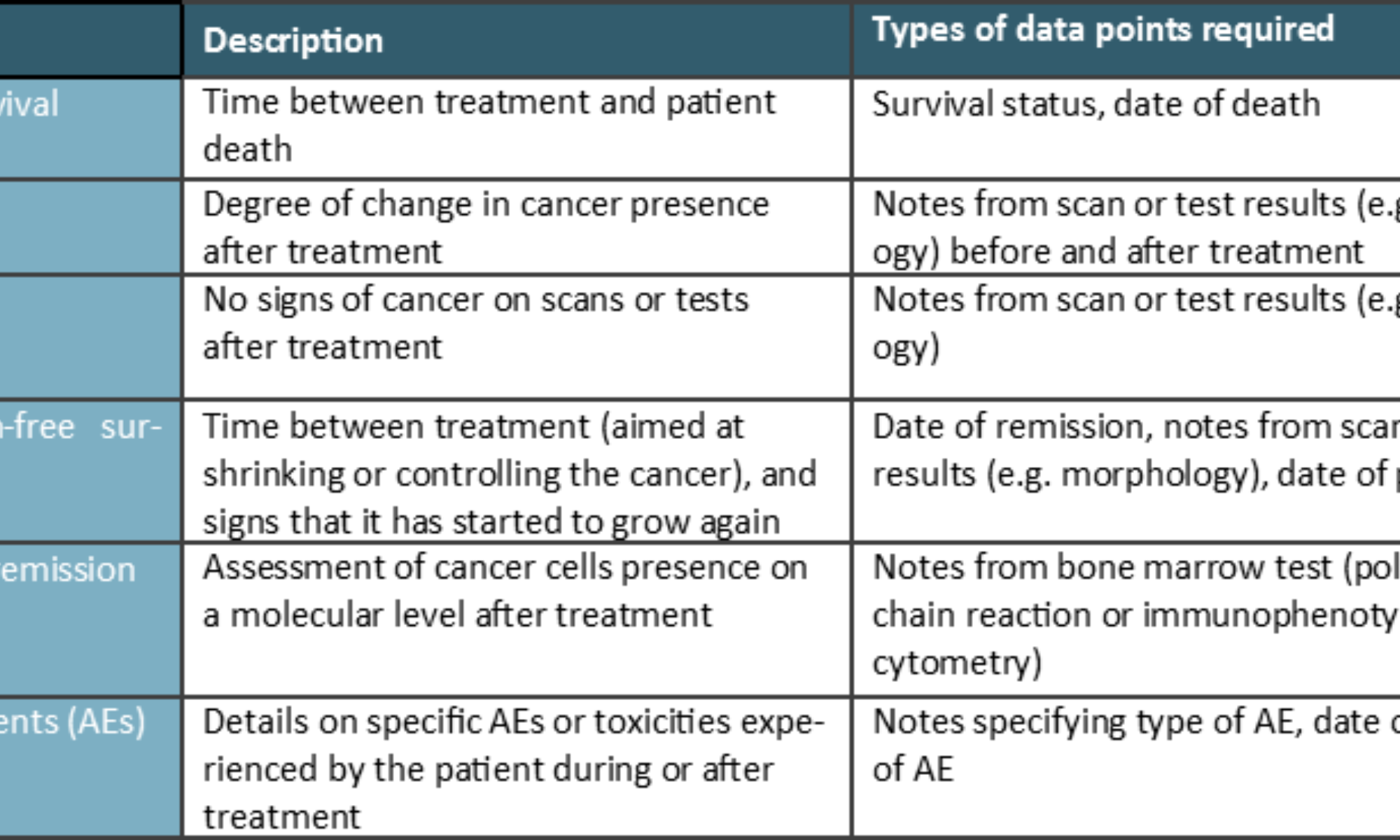
We also considered economic outcomes, e.g. hospital admissions, and healthcare resource utilisation, as well as and humanistic, patient-reported experience or outcomes measures (PREMs or PROMs) such as quality of life (QoL) and patient satisfaction.
We applied secondary and primary research to explore these issues:
- Secondary (desk) research: An assessment of the guidance documents, data collection forms and data completeness reports available in the public domain
- Primary research: interview with SACT experts to validate secondary research findings and to bridge information gaps
Findings
The SACT dataset is part of the National Cancer Registration and Analysis Service (NCRAS) within Public Health England (PHE), which aims to collect data on all cases of cancer that occur in people living in England to support public health, healthcare and research. SACT comprises several data categories, including patient demographics and consultant details, clinical status, programme and regimen details, cycle information, drug details and outcomes. It is mandatory for hospital trusts administering cancer medicines to submit data to SACT, and 141 hospital trusts upload data on a regular (monthly) basis.
Whereas it is mandatory for trusts to submit data to SACT, not all the data fields within the SACT data collection form are mandatory to fill out. The SACT form includes fields that are ‘Mandatory’, ‘Required’, ‘Optional’ and ‘Pilot’. ‘Mandatory’ fields have to be completed in order for the submission to be accepted; ‘Required’ fields must be included “where available or applicable”; ‘Optional’ fields are discretional. The SACT data collection form was revised in 2018, and the new form is set to be implemented in December 2019.
Since the revised SACT form has not yet been implemented, there is no completeness data available for it, however, there is historical data (from previous versions of the SACT form) available in annual reports. In the figure below, we present completeness rates for select data fields collected through SACT in 2017-18, focusing on the data fields that are likely to be of greatest use for enabling OBR for cell and gene therapies (with data labels highlighting the completeness rates for data fields that are of particular relevance for OBR).
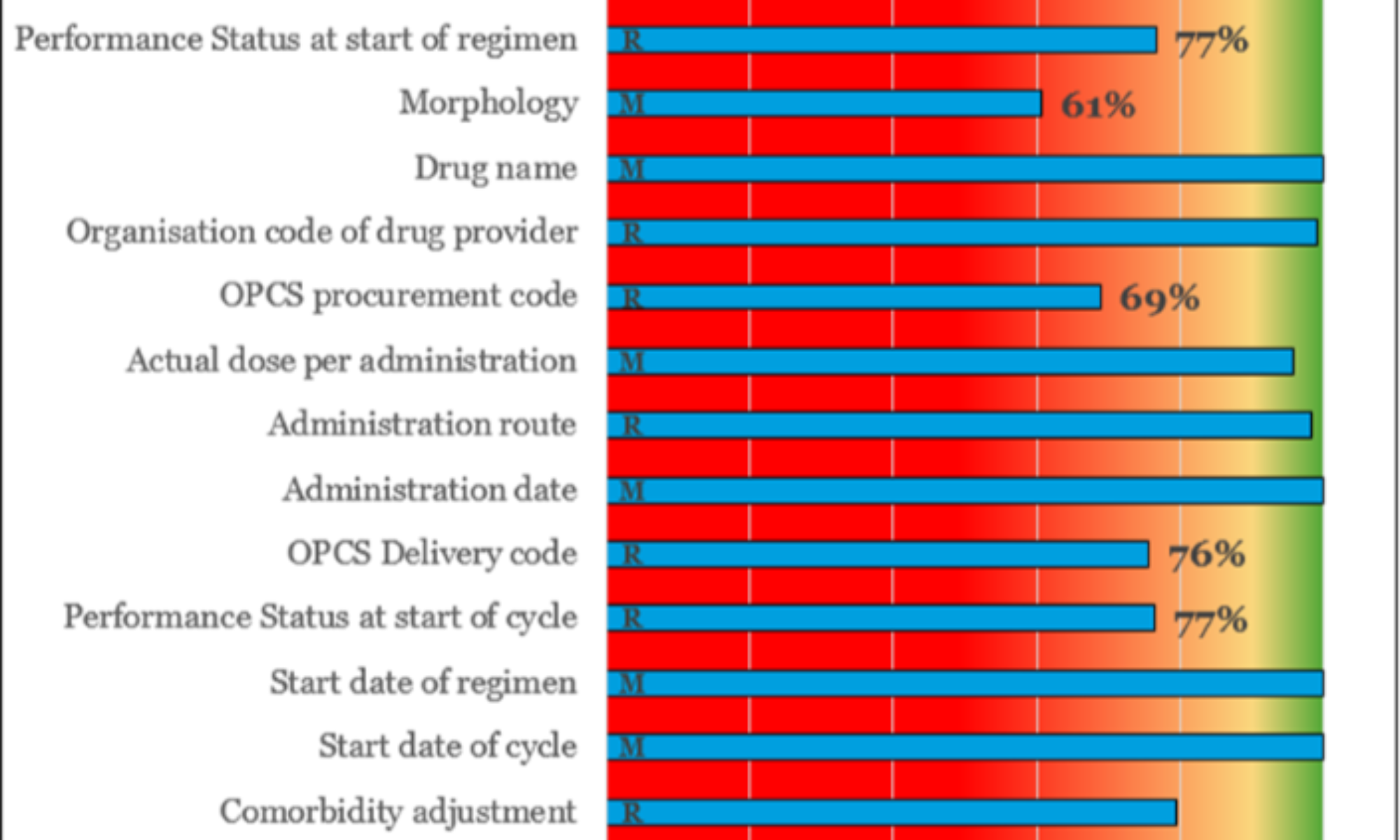
Overall, there is a substantial spread in the results (ranging from 12% to 100%), but interestingly, the data fields that we have identified as being of greatest potential use for OBR (indicated with data labels in the figure above), are all below 80% completeness, with a mean across them of 58%. Most notable is the completeness rate for the regimen outcomes summary, which is perhaps the most relevant for OBR, with a mean completeness of only 12% across trusts in England (median of 7%).
Another striking feature of the SACT completeness data is the difference between the ‘Mandatory’ (i.e. have to be completed in order for the submission to be accepted), and ‘Required’ (must be included “where available or applicable”) data fields; ‘Mandatory’ entries have an average completeness rate of 96% (99.6% when adjusting for the one outlier), while ‘Required’ fields score 82% on average.
Clinical outcomes
Our research found that none of the clinical outcomes listed in the table above can be captured in SACT. More specifically:
- Overall survival (OS): OS can no longer be tracked after the field for ‘Date of death’ was removed in the 2018 update, however, this data can be obtained separately from the Office for National Statistics (ONS).
- Response: The updated SACT form includes a field for morphology at the start of treatment, which allows for part of the response outcome to be collected (morphology at baseline). Importantly, since there is no field for entering the morphology at the end of the treatment, it is not possible to systematically track morphological changes (i.e. Response).
- Remission: There is no field detailing remission or scan or test results post treatment, however, the ‘Outcomes summary – Curative’ field could potentially be used as a proxy. It is important, however, to note that this is not a ‘Mandatory’ field, and the that the mean completeness rate of 12% (median of 7%) from 2017-18 renders it of little practical value.
- Progression-free survival (PFS): The outcomes summary allows users to indicate whether the treatment regimen was stopped due to ‘Progressive/recurrent cancer’, however, this relates only to the time span of the treatment regimen, and importantly does not specify the date of remission, meaning it is not possible to capture PFS. Additionally, there is no field for capturing scan or test results post treatment, which is a further barrier to capturing PFS. Finally, the issue around completeness for the outcomes summary apply also here.
- Molecular remission: SACT does not include fields that capture the test results needed to detail molecular remission.
- Toxicities/adverse events: SACT does not capture specific information regarding toxicity or adverse events, it can only be used to determine whether toxicity was a reason for discontinuing treatment.
SACT’s gaps are substantial in terms of collecting the data necessary to capture most of the key clinical outcomes used in cancer. Some of the missing data points can potentially be retrieved from the Electronic Health Records (EHRs) or some of the other data sources that feed into NCRAS (e.g. Hospital Episode Statistics, and/or the Office for National Statistics) using the NHS patient identification numbers, however, this requires integrating SACT with additional data sources, as well as overcoming governance issues (e.g. EHR data are under the governance of individual trusts).
Economic outcomes
SACT does not capture economic outcomes like hospital admissions (inpatient or outpatient), the cost of the drugs or procedures involved, or any other detail on health resource utilisation beyond the dosages used. Costs and resource utilisation data is possible to collect through other sources, e.g. the Hospital Episode Statistics, or Secondary Uses Services using the NHS patient identification numbers, however, this requires investment in systems integration, as well as overcoming governance issues.
Humanistic outcomes
QoL outcomes are not captured in SACT, whether disease-specific or generic. SACT includes entries for a patient-reported functional outcome, i.e. ‘Performance status at the start of treatment’ (regimen and cycles), which uses a WHO measure from 0-4, detailing patients’ ability to carry out normal daily activities like work and self-care. However, there is no field collecting information about performance status after treatment, which means it is not possible to track improvements post treatment.
PROMs and PREMs such as ability to return to normal daily activities are increasingly regarded as important, perhaps especially for younger patients, however, there are two key issues relating to collecting PROMs/PREMs. Firstly, that there is no currently agreed standard or consensus on what PROMs and PREMs are most relevant in cancer, so this would have to be defined in advance, and secondly, that there is no existing databases currently used across the NHS nationally that can be leveraged, so this would have to be resolved as well.
Implications
On the face of it, SACT appears well-placed to facilitate OBR in cancer as it has a very high number of English trusts contributing to it, and is run by a trusted national body (Public Health England). However, our gap analysis shows that SACT, in isolation, is largely unfit as a framework for enabling OBR, and that significant upgrades and integration with other data sources are required.
Importantly, SACT does not allow for a systematic tracking of key clinical outcomes used in cancer such as OS, PFS, response or remission, which means that additional data needs to be collected either through new data fields in SACT or from other sources (e.g. electronic health records) to enable OBR. Some of this additional data could potentially be collected through NCRAS, however, this increases complexity as it requires integration between different data sources.
We believe that establishing a data collection infrastructure that can facilitate OBR through clinical, economic and/or humanistic outcomes is a highly desirable future goal, which can benefit patients, clinicians, researchers, the NHS and manufacturers alike. This system should be appropriately automated to reduce the burden on already thinly spread clinical staff, and scalable so that it can enable OBR not only in cancer, but also in other therapy areas. Importantly, it should provide transparency to both manufacturers and NHS stakeholders so that all parties can learn from the outcomes collected in the real world, and maintain confidence in that the financial implications (e.g. payments or rebates) represent the terms that were agreed in the reimbursement scheme.
It is particularly important to ensure that this data is a resource that clinical staff can benefit from, as such learnings encourage further improvements in patient care, as well as keeping data quality and completeness high. All stakeholders in the healthcare ecosystem win if patient outcomes are improved, and this requires a concerted effort by all stakeholders to become a reality. We believe that the time is right for this effort to be made and for the advanced therapies to be complemented by targeted and meaningful real-world data collection to enhance and incentivise quality patient care.